About the Author
Professor Thierry PASSERON is a dermatologist, academic professor and researcher who works for INSERM and based in CHU of Nice, south of France. Pr. PASSERON is a worldwide specialist in vitiligo and has been among the first users of excimer phototherapy. He ran several studies on vitiligo, psoriasis and alopecia areata using 308 nm lasers and lamps.
Abstract
Excimer phototherapy refers to dermatological treatments using the monochromatic light at 308nm. It has been introduced in the early 2000’s and is now used to treat a wide range of skin disorders such as vitiligo, psoriasis, and atopic dermatitis. This paper presents our use of excimer devices in our everyday practice at the Hospital of Nice.
Introduction
UV light is well known to have a benefic impact on many skin diseases. The mechanism of action is the reduction of T-Cell proliferation by cellular apoptosis. Among UV wavelengths, 308nm has been found to be the most effective wavelength to induce the apoptosis of lymphocytes.
The last two decades have seen significant technological advances, expanding the options for patient who needs phototherapy. Numerous clinical studies showed the efficacy of excimer in the treatment of various skin diseases including pigmentation disorders and/or inflammatory skin reaction.
Material
The dermatology department of the university hospital of Nice has a long experience with UVB light. Our first excimer device was a Xenon- Chloride laser (Talos from Wavelight Aesthetic). This technology is very efficient but is also very bulky and very costly. We then switched to a handheld excimer lamp (308 from Alma Lasers) with the same clinical efficiency than our laser. We now use a smaller and much more powerful excimer lamp (Exci308nm from Aerolase). This later device is as efficient as bigger excimer devices (lasers and lamps) but treatments are faster and the Exci308 is lighter, ergonomic and much more convenient to use.
Protocol and treatment
In our experience, whatever the indication is, the best results are achieved when the UV light exposure results in a light pink erythema that last no more than 24 hours. Our usual protocol consists in finding this exact excimer dose by increasing or decreasing the delivered dose sessions after sessions.
For vitiligo lesions, we usually perform the first treatment at the starting dose of 100mJ/cm2, whatever the skin phototype of the patient. This dose is safe and do not lead to any side effect. We then increase the dose by 50mJ/cm2 or 100mJ/cm2 at each session until we reach the expected endpoint. The delivered dose is then stabilized and the treatment is continued until patient satisfaction is achieved or no more improvement is visible.
To treat psoriatic patients, the same protocol is used but the starting dose depends on induration. We usually start with a dose equal to 3 minimal erythema dose (MED) and increase by 0.5 or 1 MED depending on the result of the previous session.
MED test might be useful in early stages of excimer therapy, but is no longer performed in our practice. Indeed, with practitioner experience, using skin phototype and location of the lesion to treat are enough to determine the required dose.
The side effects include erythema and transient perilesional hyperpigmentation. Higher doses sometimes lead to blisters with our laser on psoriasis lesions. We now gave up doing very aggressive protocols (10 MED).
When possible, treatment is performed twice a week. It has been shown that the efficiency of the treatment depends on the total number of sessions rather than on frequency. Twice a week appears to be the best compromise for fast improvements and low side effects.
Therapeutic indications
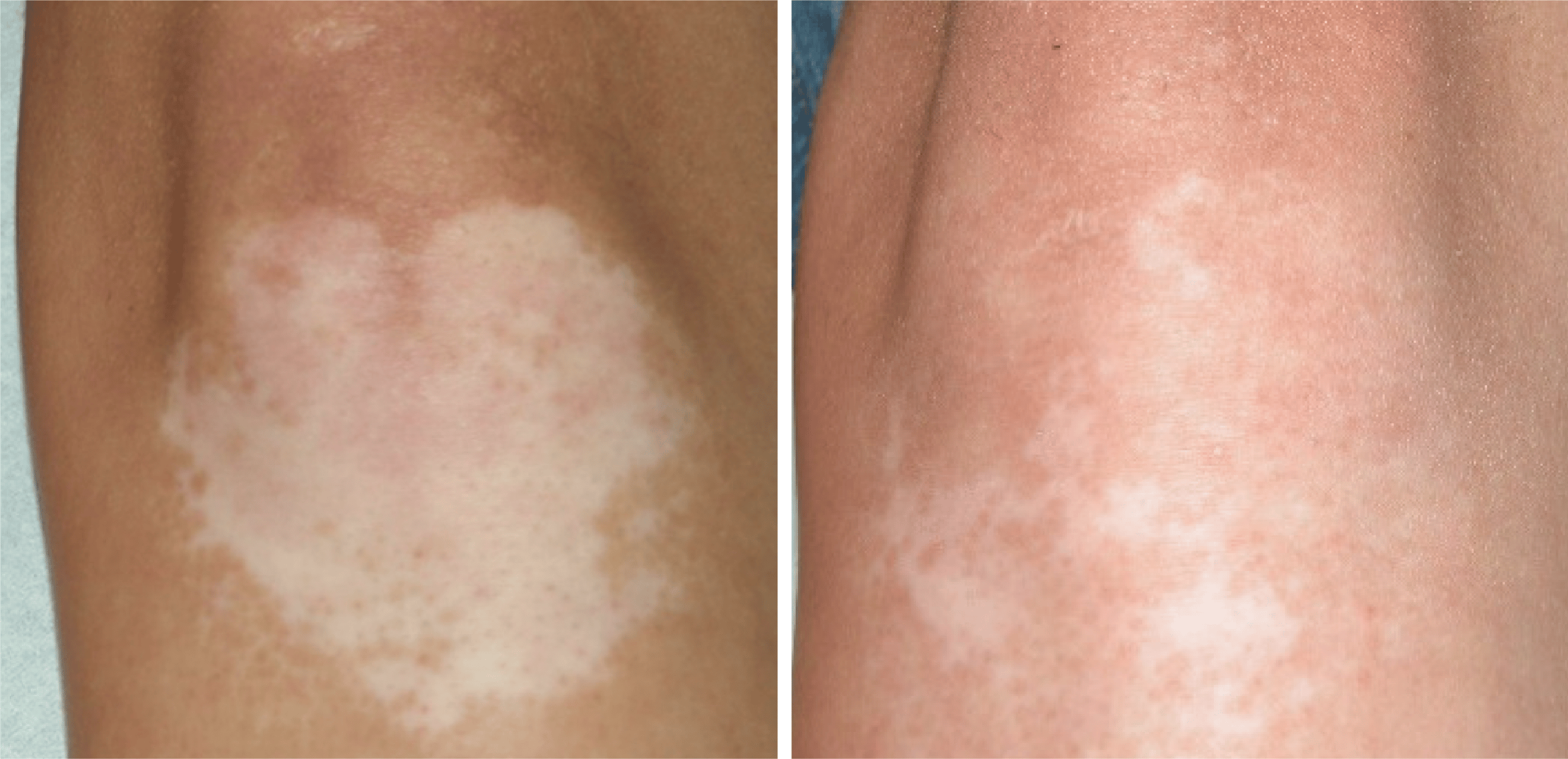
Vitiligo is probably the best indication for excimer phototherapy devices. The localized exposure associated with the best wavelength gives excellent results. We showed in a previous study that the excimer laser and excimer light are equivalent in terms of efficacy and safety and are better than Nb-UVB. Nevertheless, improvement highly depends on the treated area. Most of the time, a complete regimentation is observed on the face when Exci308 is used in combination with Tacrolimus 0.1% or Pimecrolimus 1% twice a day. Good results are also observed on neck or trunk. Fingers and toes respond less to treatment, including excimer light. During the treatment, it is important to expose the edges of the white patches to stimulate the migration of the surrounding melanocytes.
In our practice, Exci308 phototherapy is used in combination with topical treatment for localized vitiligos.
Psoriasis is a well-recognized indication for excimer devices. Many studies have been published and show excellent improvement in PASI score. In our practice at the university hospital, we use excimer phototherapy only as second line treatment for psoriasis. It is often very efficient to cure hard-to-treat remaining lesions. For these difficult cases, it is helpful to diminish the flakes with a salicylic acid based cream and to perform the treatment in association with topical steroids.
The delivered excimer dose for psoriasis is much higher compared to other indications. It can reach 6 to 7 times the MED. For this level of treatment intensity, it is very preferable to use a powerful device with a large spot size but surrounding healthy tissues must be perfectly protected!
In the dermatology department, we also use the Exci308 for Leukoderma (post-surgical, post- CO2 laser, post-cortisone injection, etc.) with encouraging results that need to be maintained with spaced complementary sessions. We also got an excellent response on Lichen amyloidosis for which dermatologists rarely have a treatment to offer.
Conclusion
Exci308 phototherapy is very useful in our everyday practice. It is not only a well-demonstrated effective and safe treatment for vitiligo and to a lesser extent for psoriasis. Most of the time, it can be combined with other therapies to optimize the clinical results.
Exci308 phototherapy has zero running cost and can be performed by doctors or nurses in a very short time. It is therefore an important equipment for phototherapy dermatologists of our department.