Treatment Update for Mild to Moderate Psoriasis
A recent study shows that the efficacy and tolerance of a 650-microsecond 1064-nm laser is equivalent to that of the 308-nm excimer laser for the treatment of mild to moderate psoriasis of the extremities. The 650-microsecond laser can also be used in combination with a biologic medication and in patients with dark skin without cooling during treatment.
Neo Elite vs. Excimer Laser
It’s well known that phototherapy is effective against psoriasis and lacks the side effects of systemic medications1. For plaque psoriasis, the 308-nm excimer has been considered first-line phototherapy1–8. Nestor and colleagues9, in their randomized, investigator- blinded study, compared the efficacy and tolerability of a new device, the 650-microsecond, 1064-nm pulsed YAG laser (Neo® Elite, Aerolase Corp., Tarrytown, NY), to that of the excimer laser (XTRAC Velocity 400®, PhotoMedex, Inc., Montgomeryville, PA) for the treatment of mild to moderate psoriasis vulgaris of the arms and legs. The authors treated plaques on one side of the body with the Neo Elite and plaques on other side with the 308-nm excimer laser. They found that redness, thickness, scaliness, mPASI (Psoriasis Area Severity Index) scores for arms and legs, and overall mPASI scores did not differ significantly for the treated psoriatic plaques on each side of the body. They also reported that scores for erosion/ulceration, vesicles, erythema, scaling, edema, and atrophy were low and identical for both devices. The authors concluded that the efficacy and tolerance of the Neo Elite are equivalent to that of the excimer laser for the treatment of mild to moderate psoriasis vulgaris of the arms and legs.
Since reporting these findings, Nestor and colleagues have added that the Neo Elite also provides significant clearance in thicker psoriatic skin areas, even on recalcitrant cases of the hands and feet, sometimes in just several treatments.
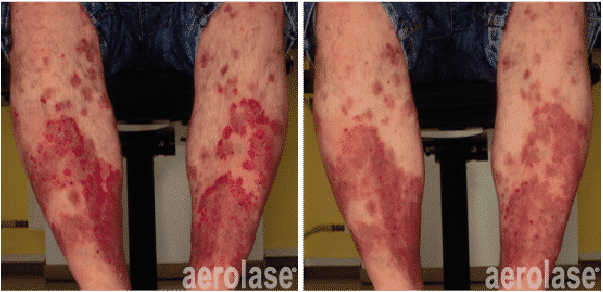
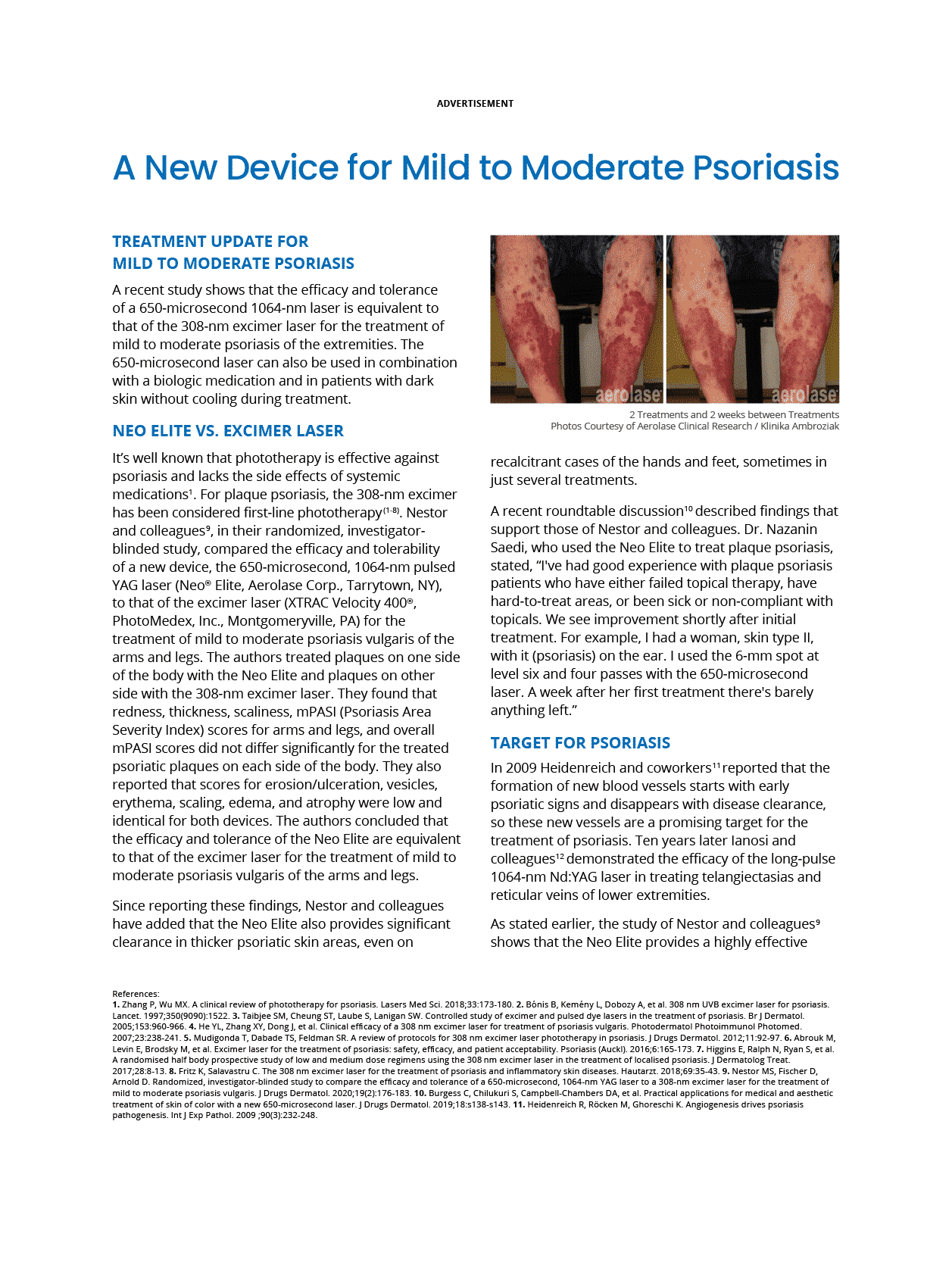
2 Treatments and 2 weeks between Treatments. Photos Courtesy of Aerolase Clinical Research / Klinika Ambroziak.
A recent roundtable discussion10 described findings that support those of Nestor and colleagues. Dr. Nazanin Saedi, who used the Neo Elite to treat plaque psoriasis, stated, “I’ve had good experience with plaque psoriasis patients who have either failed topical therapy, have hard-to-treat areas, or been sick or non-compliant with topicals. We see improvement shortly after initial treatment. For example, I had a woman, skin type II, with it (psoriasis) on the ear. I used the 6-mm spot at level six and four passes with the 650-microsecond laser. A week after her first treatment there’s barely anything left.”
Target for Psoriasis
In 2009 Heidenreich and coworkers11 reported that the formation of new blood vessels starts with early psoriatic signs and disappears with disease clearance, so these new vessels are a promising target for the treatment of psoriasis. Ten years later lanosi and colleagues12 demonstrated the efficacy of the long-pulse 1064-nm Nd:YAG laser in treating telangiectasias and reticular veins of lower extremities.
As stated earlier, the study of Nestor and colleagues9 shows that the Neo Elite provides a highly effective treatment option for mild to moderate plaque psoriasis. Since the 1064-nm energy is selectively absorbed by hemoglobin in deep blood vessels13,14, the Neo Elite reaches the vasculature under the psoriatic plaque, making it possible to deliver energy to hard-to-treat areas without serious adverse effects. The result is that the Neo Elite affects both superficial and deep plaque blood vessels without the bruising associated with other lasers.
Cooling not Required
Treatments with the long pulse 1064-nm laser are painful and carry a risk of thermal damage and scarring15 because the pulse duration of 1064-nm lasers is 5 to 30 milliseconds, which is higher than the 700-microsecond thermal relaxation time of skin tissue16,17. Pulse durations of this magnitude require continuous cooling of the target skin tissue to minimize damage to surrounding tissue and discomfort during treatment18.
Unlike its long pulse 1064-nm counterpart, Neo Elite does not require cooling during treatment. The pulse duration is shorter than the thermal relaxation time of both skin and blood vessels, so the therapeutic target is heated more rapidly than the rate that heat moves to the surrounding skin, thus lowering the risk of damage and pigmentary changes19.
The Neo Elite also delivers energy in a collimated beam, so the operator may vary handpiece-to-skin distance without changing the fluence. This enhances both efficacy and safety during treatment and renders treatment less dependent on operator technique19.
Combination with Biologics
The Neo Elite has also been used in combination with biologic therapies for psoriasis. In a recent study 20, 34 patients with severe plaque psoriasis were treated at weeks 0, 4, 16, and 28 with ustekinumab (Stelara®, Jansen Biotech, Inc., Horsham, PA) followed by eight Neo Elite treatments, 3 to 4 passes at 25–28 J/cm2, at 1-week intervals. PASI and BSA (Body Surface Area) scores were evaluated after completion of biologic therapy and after the final Neo Elite session.
After biologic therapy alone, the average values were PASI 75 and BSA 8. At the end of Neo Elite therapy, the average values were PASI 90–100, and BSA 2–0. Adverse events were not observed and tolerability was high during the entire study. The authors concluded that the Neo Elite device improved both PASI and BSA scores achieved with biologic therapy alone.

2 Treatments and 2 weeks between Treatments. Photos Courtesy of Aerolase Clinical Research / Klinika Ambroziak.
Skin of Color
The Neo Elite can also be used to treat patients with dark skin. The pulse duration is shorter than the thermal relaxation time of both the blood vessels and the skin, so the target is heated more rapidly than the rate that heat is conducted to the surrounding skin. This reduces damage and lowers the risk of pigmentary changes18–21. With its 650-microsecond pulse duration, the Neo Elite’s infrared 1064-nm energy also lacks the increased risks of skin cancer and skin aging linked to UV lasers.
These studies and others have resulted in FDA clearance of the Neo Elite for the treatment of psoriasis.
References
1. Zhang P, Wu MX. A clinical review of phototherapy for psoriasis. Lasers Med Sci. 2018;33:173-180.
2. Bónis B, Kemény L, Dobozy A, et al. 308 nm UVB excimer laser for psoriasis. Lancet. 1997;350(9090):1522.
3. Taibjee SM, Cheung ST, Laube S, Lanigan SW. Controlled study of excimer and pulsed dye lasers in the treatment of psoriasis. Br J Dermatol. 2005;153:960-966.
4. He YL, Zhang XY, Dong J, et al. Clinical efficacy of a 308 nm excimer laser for treatment of psoriasis vulgaris. Photodermatol Photoimmunol Photomed. 2007;23:238-241.
5. Mudigonda T, Dabade TS, Feldman SR. A review of protocols for 308 nm excimer laser phototherapy in psoriasis. J Drugs Dermatol. 2012;11:92-97.
6. Abrouk M, Levin E, Brodsky M, et al. Excimer laser for the treatment of psoriasis: safety, efficacy, and patient acceptability. Psoriasis (Auckl). 2016;6:165-173.
7. Higgins E, Ralph N, Ryan S, et al. A randomised half body prospective study of low and medium dose regimens using the 308 nm excimer laser in the treatment of localised psoriasis. J Dermatolog Treat. 2017;28:8-13.
8. Fritz K, Salavastru C. The 308 nm excimer laser for the treatment of psoriasis and inflammatory skin diseases. Hautarzt. 2018;69:35-43.
9. Nestor MS, Fischer D, Arnold D. Randomized, investigator-blinded study to compare the efficacy and tolerance of a 650-microsecond, 1064-nm YAG laser to a 308-nm excimer laser for the treatment of mild to moderate psoriasis vulgaris. J Drugs Dermatol. 2020;19(2):176-183.
10. Burgess C, Chilukuri S, Campbell-Chambers DA, et al. Practical applications for medical and aesthetic treatment of skin of color with a new 650-microsecond laser. J Drugs Dermatol. 2019;18:s138-s143.
11. Heidenreich R, Röcken M, Ghoreschi K. Angiogenesis drives psoriasis pathogenesis. Int J Exp Pathol. 2009 ;90(3):232-248.
12. Ianosi G, Ianosi S, Calbureanu-Popescu MX, et al. Comparative study in leg telangiectasias treatment with Nd:YAG laser and sclerotherapy. Exp Ther Med. 2019;17(2):1106-1112.
13. Prieto V, Zhang P, Sadick NS. Comparison of a combination diode laser and radiofrequency device (Polaris) and a long-pulsed 1064-nm Nd:YAG laser (Lyra) on leg telangiectases. Histologic and immunohistochemical analysis. J Cosmet Laser Ther.2006 Dec;8(4):191-195.
14. Yang J, An X, Li Y, Tao J. Multi-wavelength laser treatments of spider nevi. Lasers Med Sci. 2019;34(4):737-742.
15. Adamič M, Pavlović MD, Troilius Rubin A, et al. Guidelines of care for vascular lasers and intense pulse light sources from the European Society for Laser Dermatology. J Eur Acad Dermatol Venereol. 2015;29(9):1661-1678.
16. Hochman LG. Laser treatment of onychomycosis using a novel 0.65-millisecond pulsed Nd: YAG 1064-nm laser. J Cosmet Laser Ther. 2011;13: 2-5.
17. Walsh JT Jr, Flotte TJ, Anderson RR, Deutsch TF. Pulsed CO2 laser tissue ablation: effect of tissue type and pulse duration on thermal damage. Lasers Surg Med. 1988; 8:108-118.
18. Gold MH, Goldberg DJ, Nestor MS. Current treatments of acne: Medications, lights, lasers, and a novel 650-μs 1064-nm Nd: YAG laser. J Cosmet Dermatol. 2017;16(3):303-318.
19. Roberts WE, Henry M, Burgess C, et al. Laser treatment of skin of color for medical and aesthetic uses with a new 650-microsecond nd:yag 1064nm laser. J Drugs Dermatol. 2019;18:s135-s137.
20. Evgenievna M., Sergeevna K., Vladimirovna I. Systemic biologic therapy combined with a 650-microsecond laser for patients with severe forms of psoriasis. Presented at ASLMS 2019.
21. Rose AE, Goldberg DJ. Successful treatment of facial telangiectasias using a micropulse 1,064-nm neodymium-doped yttrium aluminum garnet laser. Dermatol Surg 2013; 39: 1062-6.


